COVID-19 has provided a useful lens through which to examine the capacity of counties to cope or break under the stress of this uniquely severe health crisis. While devolution is still nascent and while it must be recognised that no institution could possibly be prepared for a pandemic of this scale, yet even at this early stage a clear pattern is emerging; northern counties are poorly prepared for large-scale epidemics because of large-scale corruption and mismanagement.
When the novel coronavirus hit Kenya, it prompted a national stocktaking. It emerged that in northern Kenya there is only one county with a functionally equipped Intensive Care Unit (ICU). Eight years after devolution; this is an inexcusable dereliction of duty.
For almost 50 years of Kenya’s independence, the stock-in-trade of northern Kenya’s political elite was to blame the region’s underdevelopment on the central government’s failure to allocate adequate resources to the region. Everything could be packed into a convenient single narrative: we are marginalised by the central government. As a result, the political elite hardly took responsibility for their failure.
If marginalisation was caused by the national government’s failure to allocate adequate resources, significant amounts of money have been allocated to the counties under devolution, money which, had it been optimally used, could have transformed the fortunes of these counties.
Devolution as an antidote
Sirkal Saidia, government to the rescue, was the modus operandi of the leadership in northern Kenya, a call mostly made when an official from the national government visited. It was pervasive during President Daniel Moi’s era; at public rallies, a leader’s eloquent narration of the problems facing the area was celebrated and in fact recognised as the hallmark of a good leader.
This turned visits by former president Moi or other powerful political leaders into a spectacle as local leaders attempted to outdo each other in presenting the laundry list of problems afflicting the region. The list would always include a road here, a school there, and a hospital in between, that required fixing through the goodwill of the visiting national government official.
But central to devolution was bringing resources and power to the counties and hence closer to the people. This was heralded as the antidote to the decades of marginalisation. Yet eight years after devolution, the level of development does not match the resources allocated. There are of course areas where things have improved but overall, devolution has merely spawned a phalanx of local extractive “tender mafia networks” that have captured these marginalised counties and continue to subvert the benefits of devolution.
For the average citizen, the only thing that has changed is that their marginalisation now has a local flavour. The money meant for them has created overnight millionaires who are putting up all manner of grotesquely designed vanity projects like multiple-bedroom houses without electricity, marrying second/third wives, and purchasing vehicles worth many times the salaries of county officials. Some are so brazen that they flaunt their newly acquired wealth, a case of eating with their mouths open.
There are deep parallels between how the Kenyan state was imposed from the top as a control tool, and how the county governments, with a few shrewd “businessmen”, determine what gets done or not. Devolution is moored not to the constitutional provisions or even the needs of the citizens but to these men. Devolution was reimagining governance away from the centralised, colonial, top-down extractive state—which gave way to the centralised post-colonial state— and towards a more bottom-up, people-friendly, accountable model.
But in northern Kenya, that vision has been perverted. The elite are engaged in industrial-scale corruption that makes the corruption of the pre-devolution days look like child’s play. Before devolution, the gripe was that those engaged in corruption were civil servants from southern Kenya who were not locals, for instance, junior civil servants deployed to Marsabit who owned top of the range vehicles which they would park in Isiolo, mwisho wa lami, from where they would be driven to Marsabit by a government driver, (probably a local) in a government vehicle, returning to their cars in Isiolo to drive home at the end of the day.
This was always rationalised as the behaviour of outsiders who cannot be deterred by social shame. But with devolution, and because of the weakness of the county governments, especially the governors, corruption has become deeply entrenched and the prime beneficiaries are the local political elite. In one case, a former governor had the government’s Integrated Financial Management Information System (IFMIS) installed in his bedroom rather than at the county office. This has eroded the trust and legitimacy of county government institutions.
In northern Kenya, as elsewhere, corruption has become the central activity with all its elaborate bureaucracy, processes and structures, and deception is used to make it look like a government process. The present pandemic, combined with a cholera outbreak in one corner, floods in another corner and locusts in yet another, has revealed how ill-prepared the counties are and by the same token also revealed the cost of corruption, leaving the Marsabit, Turkana and Mandera governors with no place to hide.
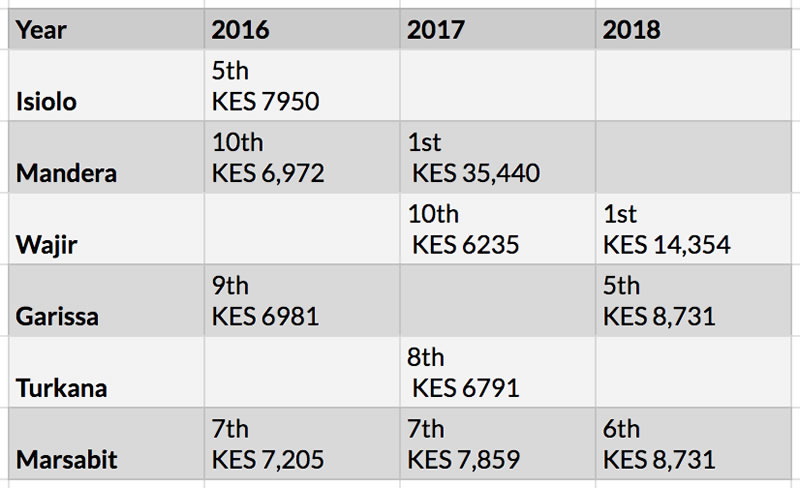
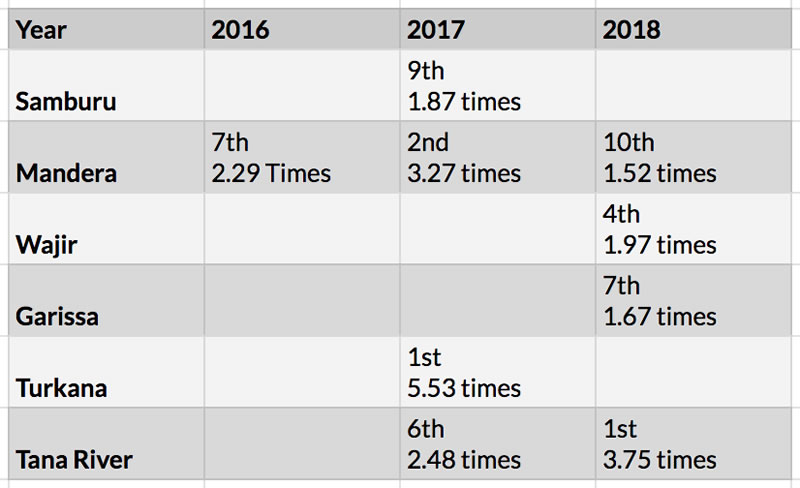
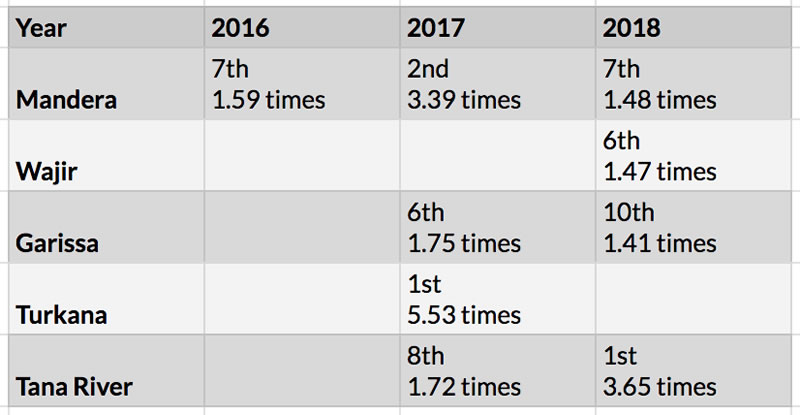
Northern Kenya counties feature prominently in the list of most corrupt counties produced by the Ethics and Anti-Corruption agency. Four counties in the region consistently among the top 10 most corrupt counties in Kenya when these three forms of corruption are considered: top ten counties by proportion of those who paid bribes, top ten counties by average number of times a bribe was demanded, top 10 counties by average number of times a bribe was paid.
Top 10 counties: Amount paid in bribe
Top 10 counties: Times bribe is demanded
Top 10 counties: Times bribe is paid
COVID-19 and the health system in northern Kenya
Reports of a COVID-19 case in Mandera sent a wave of panic across the northern region. This was partly because of the general anxiety around the lack of health facilities, which makes the region a sitting duck because the health infrastructure to deal with even controllable disease outbreaks is non-existent and the resources allocated are missing.
How, despite all these limitations, the people of northern Kenya endure is a story of luck and resilience. As a mode of production, pastoralism has not relied so much on the state’s service provision. Pastoralists have bent the market to their will and survive by sheer grit by developing complex social structures of livestock redistribution systems to cushion themselves.
A certain level of baked-in fatalism in the nomadic lifestyle, some of it often buttressed by an uncritical understanding or a downright misinterpretation of Islam—death is not to be feared—has also emerged. Immediately coronavirus was announced in Kenya, some of the more memorable television interviews were of elderly Cushitic men saying that death was inevitable and so there was no need for alarm. The uncertainties produced by the nomadic environment have made pastoral communities prone to shocks and epidemics which they have recorded in elaborate oral narratives. For example, the Gabra people have recorded all livestock and human diseases in the names of the years the epidemics occurred. Whenever epidemics erupt, past effects and coping mechanisms are revisited.
The ailing health sector
The healthcare infrastructure in most of northern Kenya survived on the benevolence of Christian missionaries’ networks of hospitals, dispensaries, and medical clinics spread across the region. Following devolution, Marsabit county government initially recognised the complementary role of the mission hospital, but as the years went by the county government sought to supplant the missionary investment by building their own hospitals in close proximity. The death of mission hospitals and the emergence of more but poorly equipped, ill-staffed, and poorly managed health facilities have contributed to the conundrum currently facing the north.
The number of dispensaries is a different matter; most of them are not operational. A key medical staffing officer recently acknowledged that Marsabit County alone needs at least 1,000 more staff to operationalise many of its newly built health facilities.
Data shows that northern Kenya has the lowest percentage distribution of health professionals with the number of doctors, nurses, and clinical officers being 2%, 2%, and 5% respectively.

Public health, corruption, and unsound investment
Most of the disease outbreaks in northern Kenya fall within the public health domain rather than clinical or veterinary medicine. Public health in Kenya has suffered since it was collapsed into a department under the Ministry of Health
There have been occasional outbreaks of viral diseases and epidemics in Marsabit county. Ebola, MERS, Rift Valley Fever and Zika virus have also been reported as being present in camels and bats in the vast county. However, the county lacks even the most basic public health infrastructure and in Isiolo, even old quarantine facilities like the Tuberculosis Village have been taken over by the county government. COVID-19 should have found a better health infrastructure. Marsabit takes its blood to Eldoret for testing. Even the limited available health infrastructure is saddled with corruption, poorly prioritised investments, and a lack of a sound turnaround plan which has further compounded the problem.
One year ago, a court ruling froze the account of an Isiolo businessman who had received Sh80 million by defrauding taxpayers allegedly through the construction of two oxygen plants in 2017 “yet no such facility existed in the county”. The deal signed between the Isiolo county government and a private company called Living Goods thus became a serious point of contention. Petitions to the senate committee and several inquiries and amendments later, Living Goods was given the go-ahead to run the community health services in Isiolo County.
In Marsabit, the County Assembly canceled the procurement of two lifts that were to be installed in a hospital that is yet to be built. Eight years after devolution, Kiirua Mission Hospital still runs a special unit for patients from Marsabit County; the number of referrals to the hospital is alarming. The county government has also launched ambitious health-related programmes like the 10,000 households National Hospital Insurance Fund (NHIF) cover, building of health centres and one Level Four Hospital, and the 10 ambulances bought in 2015 at Sh172 million. The NHIF scheme has been largely a PR campaign and the health sector is still ailing.
Isiolo and Garissa Counties each have a Kenya Medical Training College (KMTC) but according to Marsabit’s leadership, the two institutions cannot serve Marsabit’s long-term vision of meeting its personnel needs, and so a Sh200 million medical training college is being built in Marsabit County. This project will only be viably operationalised in three to four years but given the lackluster leadership could take much longer.
Services in fits and starts
The health sector is an “essential service”, as evidenced by COVID-19, yet the manner in which devolved units in northern Kenya conceive “development” so far seems to preclude this continuous service provision resulting in a fits-and-starts healthcare service. The construction of big hospitals is a good beginning, but it is also a magnet for corruption. The bigger headache for the health sector in northern Kenya is how to strengthen service provision through the timely purchase of medical supplies, proper management of ambulance services, and proper record keeping.
The lack of basic health services is a recurring problem in almost all the counties of northern Kenya. In Mandera the county assembly health committee recently decried the lack of very basic health supplies. For a period of 9 months last year, Marsabit County lacked essential medical supplies like painkillers and antibiotics because of a Sh22 million debt to the Kenya Medical Supplies Authority (KEMSA). Marsabit joins other countries like Nairobi, Murang’a and Narok, which breached a KEMSA debt repayment agreement.
Despite the chief purpose of devolution being to bring resources closer to the people, vestiges of marginalisation remain; distance from the centre is still a factor hindering the availability of basic health supplies. Stringent government procurement procedures are another obstacle to timely provision of supplies, as well as lack of qualified staff in the region to maintain an inventory of medical needs.
Additionally, despite the development of health service infrastructure, private interest is visible across northern Kenya with private clinics, maternity, and private hospitals run by health personnel most of whom are employed in public hospitals. This blurring of lines between the public sector and the private sector has turned patients into customers or clients, just like at the national level. Moreover, in northern Kenya medical doctors eventually run for elective office; Dr Mohammed Kuti, the governor of Isiolo County is a trained surgeon, and is a member of COVID-19 Control Committee, while his deputy Dr Abdi Ibrahim Issa is a medic. In neighbouring Marsabit, medical doctors ran for office as Members of Parliament.
The challenges facing the northern region are myriad but the issues raised here should not be understood as constituting a case against devolution but rather an argument for better devolution.






