Abraham Maslow once said that to those who only have a hammer, the whole world looks like a nail. The reactions of world governments to the coronavirus pandemic is proof of this. Around the globe, it appears that a one-size-fits-all basket of prescriptions – from closing borders to locking down societies – seems to be all the rage. Catchphrases like “social distancing” and “self-quarantine” abound in international media reports and political speeches and proliferate all over social media.
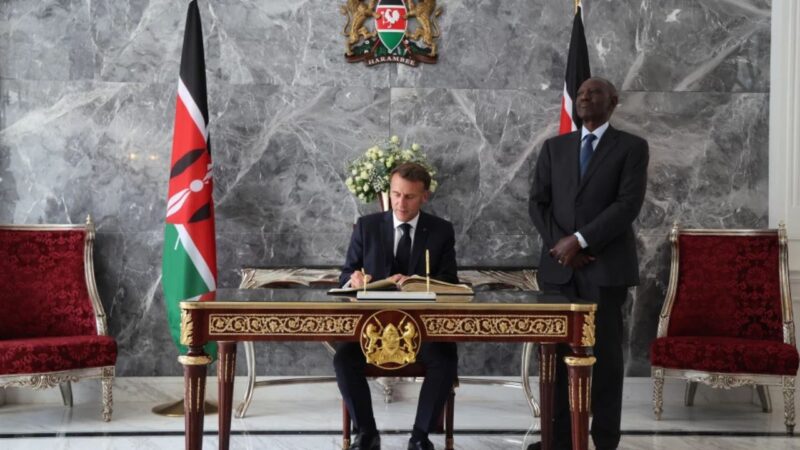
Not to be left out, African governments have followed suit. Last week, the Kenyan president, Uhuru Kenyatta, ordered all schools closed, forbade entry into the country to all but a few foreigners with residence permits and urged citizens to work from home, to wash and sanitise their hands, and to avoid crowding in public spaces, including transport. A few weeks ago, these measures would have seemed extreme. But not today, as the global advance of the virus sparks a stampede for the global system’s exits.
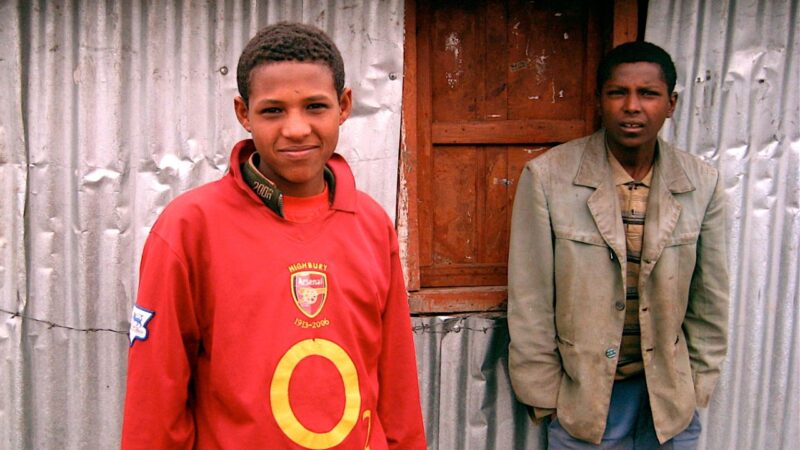
However, while the government’s rhetoric may make sense when viewed from a public health perspective, a closer look reveals the dangers inherent in blindly following the crowd. Take, for example, the situation in the Kenyan capital, Nairobi. Here, two-thirds of the city’s 4.4 million people are crammed into informal settlements, which cover just 6 percent of its land area. Within these crowded slums, entire families are forced to share single-room dwellings. With no running water, conditions are unsanitary and disease is rampant. Many slum residents work in the informal economy, running small businesses or providing casual labour to nearby rich and middle-class housing estates or to factories in the industrial areas. Few have job security or get sick leave.
The city’s public transport system is similarly crowded, unsanitary and chaotic. It is dominated by matatus – privately owned minibuses in which passengers are routinely packed shoulder to shoulder for journeys that, thanks to the city’s horrendous traffic, rarely last less than an hour. Another popular means of getting around are boda bodas or motorcycle taxis, where passengers share filthy helmets (when available) and can sometimes squeeze three to a bike.
In these circumstances, what do concepts such as “social distancing” mean? How practical is it to ask people to work from home? How exactly is someone who shares a single room with half a dozen other family members be expected to “self-quarantine” if they were to fall ill with symptoms associated with COVID-19? How are they to avoid infecting their neighbours or make it to the city hospitals – themselves hopelessly overcrowded and unsanitary at the best of times – without spreading the infection?
These practical considerations do not appear to have troubled President Kenyatta and his mandarins as they regurgitate the advice from the World Health Organization (WHO), which seems to take Western lifestyles as a template for life in the rest of the world. Perhaps this is because the government is fond of issuing “directives” when dealing with social issues, rather than consulting with its citizens. For example, researchers have noted that “approaches to reducing exposure to air pollution in informal settlements…have very little input from the people they target. As a result, they may have a low rate of acceptance”.
The people making decisions exhibit little awareness of or acquaintance with the realities of everyday life for the majority of urban Kenyans. Safely ensconced in their gated estates, accustomed to having the roads cleared for them and to being treated in well-equipped private hospitals (when they have opted not to fly abroad for medical treatment), these folks have no qualms about simply repeating the dictates from global elites. From where they sit, it can seem quite reasonable to propose that those in self-imposed quarantine have their own separate room and bathroom at a time when access to a flush toilet and piped water is a luxury for many of their fellow countrymen.
Public health in the colonial economy
The lack of appreciation for the circumstances of their fellow citizens stems from the fact that for over a century, Kenyan elites have been happy to exploit their poor neighbours for their cheap labour while doing little to invest in public services. The model was made during the colonial period. European authorities were not overly concerned with the health of the African population. In a 1987 paper titled “The 1920s Anti-Yaws Campaigns And Colonial Medical Policy In Kenya”, Marc Dawson notes that prior to 1920, “colonial medical officials were not responsible for the health of the bulk of the African population, only for caring for the health of government employees and European settlers and ensuring that epidemic disease did not disrupt the colonial economy”.
These practical considerations do not appear to have troubled President Kenyatta and his mandarins as they regurgitate the advice from the World Health Organization (WHO)…Perhaps this is because the government is fond of issuing “directives” when dealing with social issues, rather than consulting with its citizens.
Thus the focus of the colonial government was on ensuring that Africans did not carry diseases to work and did not threaten the health of Europeans, not that they were themselves healthy. For example, the outbreak of plague in Kisumu in the first decade of the 20th century elicited a quick response because of the potential for economic disruption, as well as the threat to the small European population. One can see a similar dynamic in the treatment of the poor in Nairobi’s slums today. Like the Africans in colonial Nairobi, their presence in the city is only tolerated because their labour is required. While typically their lives are blighted by disease and squalour, the government is not interested in them unless their illness poses a threat to the economy.
The response of the colonial authorities to the Third Plague Pandemic, which broke out of China’s Yunnan Province in the mid-19th century and spread globally via European steamships and merchant routes, is also illustrative. The pandemic reached Nairobi in 1902, where an outbreak led to the burning down of the Indian Bazaar, the city’s first business district. Nairobi would suffer frequent plague outbreaks over the next two decades. The persistence of the plague, according to Owaahh, “stimulated the first official town planning efforts for Nairobi, although most of the efforts were to segregate Indians whose sprawling townships were thought to be breeding grounds for carrier rats”.
In 1914, a report prepared by Prof. W. J. Simpson proposed not just the segregation of residential and commercial centres, but also, according to the book Indians in Kenya by Sana Aiyar, a “neutral belt of unoccupied land of at least 300 yards around European areas to ensure the healthfulness of the locality”. Following the outbreak of plague in Kisumu in December 1904, according to Health, State, and Society in Kenya by George Ndege, the Under Secretary of State for the Colonies declared that “great care should be exercised in the selection of sites for settlements, in keeping the native and European locations well apart”. Over the years, this segregation of the races has morphed into the class segregation that is a feature of Kenyan cities today.
To tackle the plague, the colonial authorities imposed harsh measures, including forced vaccinations, house burnings and quarantines. The Africans who bore the brunt of these measures were rarely consulted and quickly became loath to cooperate or to report plague cases in their homesteads, knowing it meant the destruction of their homes. This tendency to talk down to the people and to issue directives rather than consult with the citizens has been inherited by the current Kenya government.
Another colonial trait is the preference for quick, short-term fixes rather than long-term investments. When the first mass health survey of the African population was carried out in 1915 in the form of medical examinations of male conscripts for the Carrier Corps, the results sufficiently alarmed the authorities about the poor health situation in the African reserves from where they drew their labour. The main culprits were yaws and heart disease. The long term and more expensive solution would have been to improve the quality of life, especially as yaws has been described as a disease of poverty.
To tackle the plague, the colonial authorities imposed harsh measures, including forced vaccinations, house burnings and quarantines. The Africans who bore the brunt of these measures were rarely consulted and quickly became loath to cooperate or to report plague cases in their homesteads, knowing it meant the destruction of their homes.
However, while the 1920s anti-yaws campaign represented a first attempt by colonial medics to expand provision of healthcare beyond government employees to rural Africans, the government and physicians still chose to do it on the cheap. As Dawson notes, “rather than raising the living standards of the rural population (prevention), the colonial authorities tried to cure the population of yaws with injections of a drug of uncertain property”.
Similarly, to date the government has done little to raise living and sanitary standards in the slums. The big promises of slum upgrading have turned out to be little more than either looting schemes or empty talk. Many of the informal settlements that sprung up to house unwanted Africans when the colonials ran Nairobi persist to this very day. And while there will undoubtedly be a concerted effort to combat the coronavirus outbreak, it is unlikely that there will be any determined effort to improve livelihoods and eliminate slums.
The Spanish flu in Kenya
The next big foreign-born disease to hit Kenya in the colonial period was the Spanish flu, the deadliest pandemic in history. Originating in the United States and transported to the killing fields of World War I by American soldiers, the pandemic circled the globe, infecting between 3 and 5 per cent of the world’s population, including people in remote Pacific islands and the Arctic. It cut life expectancy around the world by about 12 years.
An interesting similarity with the current coronavirus epidemic is that the disease at the beginning was “mild, the mortality not unusually high”. Preoccupied with the events of the war, the first wave of the flu went largely unnoticed and it wasn’t until it started killing people in large numbers that the world paid attention. But by then it was too late. By the time it was brought under control, it had killed about 50 million people, more than had died in the war. And remember, this as all before the age of international commercial air travel.
The flu hit East Africa in two waves, the first beginning September 1918 and another in late 1919, killing at least 155,000 people, or an estimated 5.5 percent of the African population in Kenya. Again the reaction of the colonial authorities was largely driven by concerns over the loss of African labour. For example, as related by to Kirsten Moore in her 2013 paper, “Placing Pandemics: History of the 1918-19 Influenza Epidemics in Kenya and Uganda”, “the District Commissioner of Voi cited the influenza epidemic in arguments for a permanent native hospital, saying, ‘it is absolutely essential that adequate hospital provision be made to deal with sick labourers from […] Estates and Railways.’ A native hospital was up and running in Voi by 1921”. She points out that the pandemic was killing off African labour, “just as an influx of British settlers came to establish large, labour-intensive estates. Facing significant war debts and the prospect of bankruptcy, the administration depended on these new plantation enterprises to revitalise the economy”.
Again, it is clear that concern for the health of the natives was not the driving force behind the colonial provision of medical care to Africans. A century later, facing another epidemic, the Kenyan elite is showing itself to be similarly oblivious to the needs of the African majority and is really only concerned about its own economic and political interests.
Sink or swim together
Ironically, just as the colonials imported plague and influenza pandemics into Kenya, it is largely the wealthy, those with the means to travel abroad, who have brought the COVID-19 pandemic back to Kenya. Yet, as with the previous diseases, it is the poor, who did nothing to bring on the crisis, who will get to bear the brunt of both the disease and the government efforts to contain it.
However, there is a critical difference. As the pandemic exposes the systemic weaknesses in Kenya’s healthcare system, the shutdown of the global system means there is no escape for the wealthy who have profited from the plunder and neglect of public services. They will share the fate of the rest of the society. Thus, allowing the pandemic, whether through negligence or incompetence, to become established in the slums, will inevitably be fatal for the elite themselves.
A century later, facing another epidemic, the Kenyan elite is showing itself to be similarly oblivious to the needs of the African majority and is really only concerned about its own economic and political interests.
Since the virus threatens all, both rich and poor, it will require a whole society effort to confront it. Top-down directives will not suffice. In any case, after decades of hollowing out the state from within, the ability of the governing elites to enforce them is severely compromised. Thus it will be critical to work with communities to translate WHO advice into practical protocols that cater to the daily realities of the majority of the population rather than to the global imaginings of a privileged few.
In the short term, it is likely that the political elite will get its act together and do what is necessary to contain the pandemic. However, it is hoped that the lessons of history will not be quickly forgotten once the pandemic has passed. Maintaining a system predicated on inequality and the neglect of public services endangers everyone, not just those at the bottom of the pyramid. Kenyans, regardless of their station in life, will all sink or swim together. They can no longer afford to keep a colonial system where so few get so much at the expense of so many.